Retake
N28) Neck pain following MVC
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with neck pain.
- Review the DDx considerations in a patient with neck pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with neck pain.
History
A 42-year female patient is brought into the emergency department following a motor vehicle collision. Her head was hyperflexed after the airbag deployed, resulting in severe neck pain. Emergency services were able to promptly extricate the patient from the collision site and transport her to the hospital in a C-Collar. She denies loss of consciousness, numbness, tingling, or weakness in her limbs.
Physical Exam
Vitals: Blood Pressure: 120/80 mmHg, Heart Rate: 85 bpm, Respiratory Rate: 16 breaths per minute, Temperature: 98.6°F, Oxygen Saturation: 99% on room air.
The patient appears alert and oriented and is in a cervical collar. She exhibits severe point tenderness upon palpation of the cervical spine. However, neurological examination reveals full strength and intact sensation in all extremities. Pupils are equally round and reactive to light.
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
Severe neck pain and point tenderness following hyperextension of the neck during a motor vehicle collision most likely resulted in a cervical spine fracture.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
The patient does not meet NEXUS criteria for clearance of their C-collar as they have midline cervical spine tenderness. Therefore, they require imaging. A non-contrasted CT is sufficient for fracture and gross stability evaluation. Contrast is not strictly required considering the absence of findings suggestive of vascular injury.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Cervical spine CT
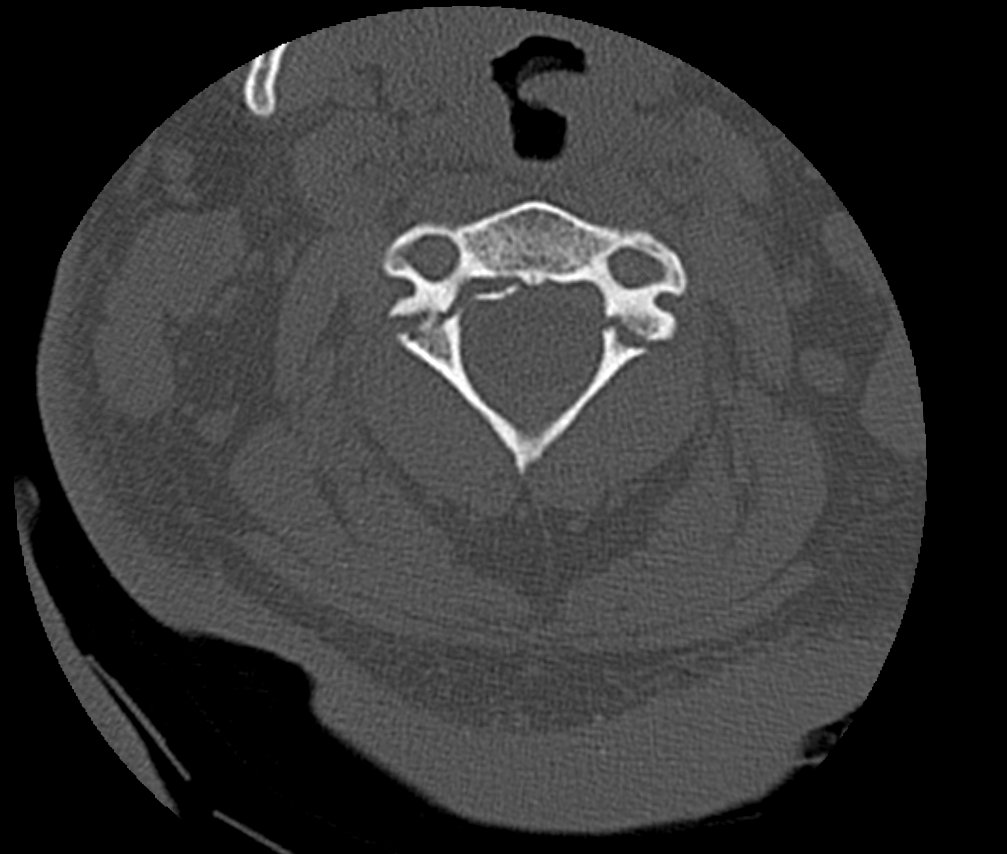
Where are the C1 fractures?
The bilateral fractures involve the bilateral partes interarticulares (plural for pars interarticularis) at the posterior arch of C1.
The fracture extends into the transverse foramina.
The transverse foramina, which house the vertebral arteries, are intact, making a vertebral artery injury less likely.
There is evidence of ligamentous injury.
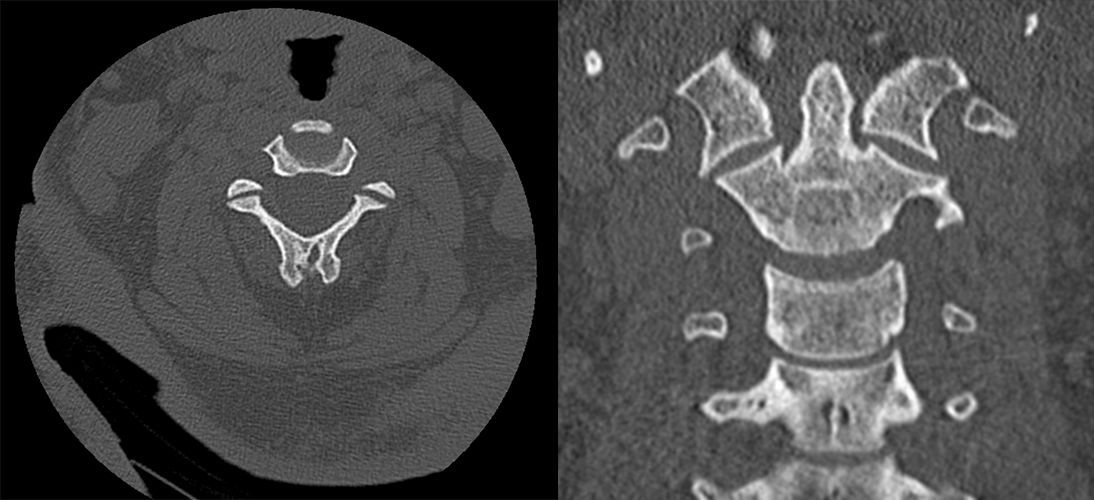
There is widening of the left C2-C3 facet joint suggesting ligamentous injury. There is also a rightward offset of the lateral masses of C1 over the dens of C2, suggesting damage of the transverse ligament, which stabilizes the dens to the anterior arch of C1.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A CTA of the head and neck is prudent in this case considering that the fracture involves the C1 vertebra. The images are not shown in this case.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
In this patient's case, the fractures at the posterior arch of C1 along with ligamentous injury, specifically the widening of the left C2-C3 facet joint and the rightward offset of the lateral masses of C1 over the dens of C2, suggest instability.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
This patient is a 42-year-old female who presents with severe neck pain following a motor vehicle collision, suggestive of a hyperflexion injury. The CT scan confirms a Hangman's fracture at C2 with evidence of ligamentous injury. Neurosurgery should be urgently consulted for potential surgical intervention. To rule out vascular injury, a CTA of the head and neck should be performed. Furthermore, an MRI might be useful for more comprehensive evaluation of the ligamentous and potential spinal cord involvement.
Lessons Learned:
- A Hangman's fracture, also known as traumatic spondylolisthesis of the axis, is characterized by a bilateral fracture of the pars interarticularis in the posterior arch of C2.
- This type of fracture typically occurs due to neck hyperextension followed by flexion, often causing injuries to the disc and posterior ligaments.
- While the primary symptom is neck pain, patients may also experience sensory loss, weakness, or paralysis following the injury secondary to spinal cord injury.
- A CT scan is typically used for diagnosis and fracture characterization.
- If the fracture extends into the transverse foramina, there's a risk of vertebral artery injury. Thus, a CTA should be performed to confirm or rule out the presence of an arterial injury. Patients with fractures involving C1-C3 should undergo a CTA.
Socioeconomic Factors: In this module, the sequence of first performing a non-contrast CT scan and subsequently a CTA of the neck was the routine approach in years past. However, practices now commonly obtain an immediate CTA of the neck in patients with suspected neck trauma. That said, it's important to note that not all patients require a CTA unless they are suspected to have blunt vascular injury (cervical bruit in young patient, expanding cervical hematoma, focal neurologic deficit, infarction, etc.) as outlined by tools such as the Revised Denver Screening Criteria, thus ensuring appropriate use of resources and reducing unnecessary radiation and contrast exposure.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}